Latest News
- 12/06/25

Correct School Uniform
Dear Families, I hope this article finds you in good health and enjoying the warmer weather. Recently, we are seeing a lot of pupils wearing non-school uniform items including hats, bracelets, hoodies, hoop earrings, extremely long nails and football tops. Please ensure you...Read Full Story - 19/06/25

KS Class Trip to Windsor
We walked to the castle, the King was in residence as the Royal Standard flag was flying. We ate a delicious ice cream. We looked at the ‘crooked’ house. We saw where the King and Queen were married. We fed the swans, geese and ducks. We had a picnic in the park and played with giant sna...Read Full Story - 19/06/25

Class KS Mosque Visit
Thank you to Mansur for helping us to understand the role of the Imam and the Mosque to help our community. Mrs K Stroud Class TeacherRead Full Story - 12/06/25

From Garden to Fork: Fresh, Organic Produce in Crunchy Munchy!
Today in Crunchy Munchy, we were excited to use fresh, completely organic produce straight from our very own Royal Lane garden. The crisp, home grown lettuce in our taco salad was harvested by a dedicated team of students and staff who have nurtured the garden with great care and commitmen...Read Full Story - 12/06/25

Year 14 Visit to The Marriott Hotel
Some Year 14 students visited The Marriott Hotel last week. It was amazing to see the internships available to our students and the opportunities that are available. The students enjoyed a presentation from Mrs Simpson and two current interns in the conference suite. Then a l...Read Full Story - 12/06/25

WizeUp Sessions Empower Year 12/13 Students
This term, some of our Year 12 and 13 students took part in the WizeUp Programme, a series of engaging sessions aimed at equipping them with essential life skills for the future. The students thoroughly enjoyed the sessions, which covered a wide range of practical topics that will help them navigate...Read Full Story - 21/05/25

Pathway 1 - Centre Parcs Residential Trip
On Monday 12th May, Pathway 1 students set off on their annual residential trip to Centre Parcs. This year, many of them went for the first time and all had a fantastic time. As usual swimming was the favourite amongst all with many taking the challenge of the water slides! Pupils also...Read Full Story - 20/05/25
Enrichment - Singing and Signing
We have had fun in enrichment singing and signing to songs like; ‘Here comes the sun’, ‘Celebration’ and ‘Reach for the Stars’. We also had a go at Karaoke too. Well done to the whole group, from Mrs StroudRead Full Story - 16/05/25

Year 11 - Greenford Mail Centre visit on 13/05/2025
Year 11 students visited Greenford Mail Centre as part of a career visit to a local employer. During the visit, students and staff toured the site (production floor and warehouse) and saw various sorting machines on the production floor, such as parcels, letters and large letters. Students had the o...Read Full Story - 16/05/25

Jack Petchey Celebration of Achievement Evening
On Thursday, 1st May, our Jack Petchey Award winners were invited to a Celebration of Achievement Evening at Cineworld Ruislip. All of last year's winners were proudly presented with medals by the Mayor of Hillingdon in recognition of their...Read Full Story - 15/05/25
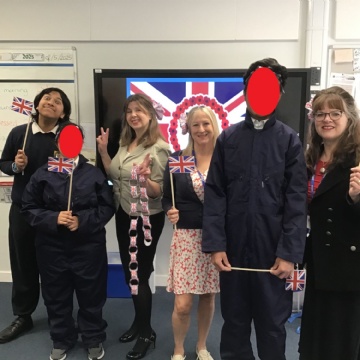
Class KS VE Day Assembly
KS class were asked to do an assembly on VE Day. We made props and decorations and dressed as pilots. We listened to the loud sirens and danced to celebrate the end of the war in Europe 80 years ago. Afterwards KS class had a small street party to celebrate. Well done to all from Mrs...Read Full Story - 08/05/25

Leading Parent Partnership Award
Leading Parent Partnership Award I am delighted to share with you that we have been awarded the Leading Parent Partnership Award (LPPA). We identified our work and relationships with families as an area for development two years ago and have used the LPPA framework to guide us on our journey. Tha...Read Full Story